Lost in Darkness : Africa
Swaziland has the world's highest concentration of AIDS cases. 40% of its adults are infected with HIV and despite treatments, it is expected that most of them will deteriotate to suffer from Acquired Immuno Deficiency Syndrome (AIDS) and eventually die. But not before transmitting this fatal disease to several of their tribesmen.
To put this in perspective, picture 10 of your close relatives and imagine a world in which 4 of them have AIDS and will succumb to the infection. Sad and stunning. But that is the normal, abysmal scenario in swaziland and most of sub-saharan Africa.
While the great influenza of 1918 claimed 40 million lives in a single year, AIDS had claimed 28 million lives by 2004 within a hundred years. Unlike influenza, which attacked furiously and was destroyed immediately, AIDS takes a slow, steady approach, and has eluded either a cure or a prevention for quarter of a century. And it is this peculiar character that makes HIV highly dangerous. AIDS is likely to reach the dubious distinction of being the single largest eradication threat mankind has ever faced. (This is assuming the H5N1 avian flu is controlled before it breaks out)
The high rate of errors that the virus RNA makes while transcripting itself into a DNA within a human cell results in a fast mutation rate and makes it a difficult moving target for anti-viral medications. Technicality apart, poor coverage of this epidemic in the media (just like the forgotten African genocides), a lack of initiative and money, has resulted in the disease spiralling out of control and now, AIDS threatens to wipe out half a continent. So much for global co-operatation, technological advances and level playing fields.
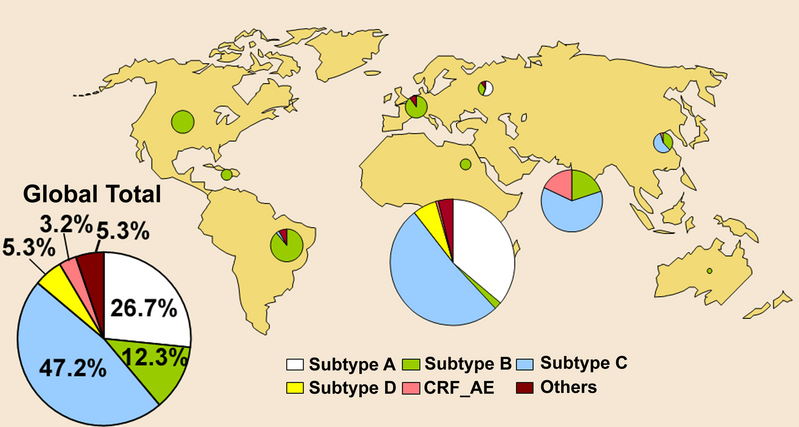
Even more stunning is the division of health budgets for fighting the virus. Most of the research in the (western) world and consequently, most of the resources humans can expend in this battle are spent in containing or finding a cure for viral strain B. But this strain affects only about 12% of the patients in absolute numbers, compared to 27% and 42% for strains A and C respectively. So, why spend all this effort on something that is only third in the list of fatal strains? Queer indeed unless you look at the global distribution of viral strains (see picture above). It now becomes clear as to why most of the efforts are spent in eliminating strain B - simply because strain B is predominantly found in the United States and Europe! Clearly, the tendency to preserve oneself comes before the desire to preserve civilization and we are presented a glorious view of global economics dictating the path to the future.
But there is still hope left. There always is. At a conference in Denver a couple of days back, Merck and Gilead Sciences have unveiled a new class of AIDS drugs, called integrase inhibitors. The drugs attack HIV's integrase, an enzyme that helps the virii merge with human DNA. Results from the preliminary tests have been spectacular - the Merck drug treated 80 patients for 16 weeks and found a majority of the patients have their virus levels drop to nearly undetectable levels. The Gilead drug treated 30 patients for 10 days. At the end of the testing, they experienced a 99% drop in virus compared to patients taking a placebo.
Although these therapies are miraculous, their long-term side effects are as yet unknown (in the short term, no side effects have been observed). Further, the HIV virus RNA has a tendency to remain inside the immune system cells without multiplication, until the cells are activated by an infection. Thus, an infected patient would require to take these medicines thoughout his life, which brings us to the next point.
No matter what the scientific advances, only those whose economic utility remains above a certain threshold will be allowed to survive. The rest have to die a protracted and painful death, consumed by the disease and more so by the torturous thoughts of an impending death. In simple terms, if the patient can make money for the drug companies or the governments that support them, they have a far higher chance of survival than the ones dependent on aid. Thus, both the AID syndromes conspire to kill a poor man. And sadly, that is not the only irony in this case.
Afterword: Read the controversy (generated by none other than the respectable organization, "Doctors without Borders") surrounding the unethical commercialization of medicines in third world countries by Gilead Sciences at http://blog.bioethics.net/2006/02/aids-drug-treatment-access-walking.html. If you have come this far, it sure will make a compelling read.
While the great influenza of 1918 claimed 40 million lives in a single year, AIDS had claimed 28 million lives by 2004 within a hundred years. Unlike influenza, which attacked furiously and was destroyed immediately, AIDS takes a slow, steady approach, and has eluded either a cure or a prevention for quarter of a century. And it is this peculiar character that makes HIV highly dangerous. AIDS is likely to reach the dubious distinction of being the single largest eradication threat mankind has ever faced. (This is assuming the H5N1 avian flu is controlled before it breaks out)
The high rate of errors that the virus RNA makes while transcripting itself into a DNA within a human cell results in a fast mutation rate and makes it a difficult moving target for anti-viral medications. Technicality apart, poor coverage of this epidemic in the media (just like the forgotten African genocides), a lack of initiative and money, has resulted in the disease spiralling out of control and now, AIDS threatens to wipe out half a continent. So much for global co-operatation, technological advances and level playing fields.
Even more stunning is the division of health budgets for fighting the virus. Most of the research in the (western) world and consequently, most of the resources humans can expend in this battle are spent in containing or finding a cure for viral strain B. But this strain affects only about 12% of the patients in absolute numbers, compared to 27% and 42% for strains A and C respectively. So, why spend all this effort on something that is only third in the list of fatal strains? Queer indeed unless you look at the global distribution of viral strains (see picture above). It now becomes clear as to why most of the efforts are spent in eliminating strain B - simply because strain B is predominantly found in the United States and Europe! Clearly, the tendency to preserve oneself comes before the desire to preserve civilization and we are presented a glorious view of global economics dictating the path to the future.
But there is still hope left. There always is. At a conference in Denver a couple of days back, Merck and Gilead Sciences have unveiled a new class of AIDS drugs, called integrase inhibitors. The drugs attack HIV's integrase, an enzyme that helps the virii merge with human DNA. Results from the preliminary tests have been spectacular - the Merck drug treated 80 patients for 16 weeks and found a majority of the patients have their virus levels drop to nearly undetectable levels. The Gilead drug treated 30 patients for 10 days. At the end of the testing, they experienced a 99% drop in virus compared to patients taking a placebo.
Although these therapies are miraculous, their long-term side effects are as yet unknown (in the short term, no side effects have been observed). Further, the HIV virus RNA has a tendency to remain inside the immune system cells without multiplication, until the cells are activated by an infection. Thus, an infected patient would require to take these medicines thoughout his life, which brings us to the next point.
No matter what the scientific advances, only those whose economic utility remains above a certain threshold will be allowed to survive. The rest have to die a protracted and painful death, consumed by the disease and more so by the torturous thoughts of an impending death. In simple terms, if the patient can make money for the drug companies or the governments that support them, they have a far higher chance of survival than the ones dependent on aid. Thus, both the AID syndromes conspire to kill a poor man. And sadly, that is not the only irony in this case.
Afterword: Read the controversy (generated by none other than the respectable organization, "Doctors without Borders") surrounding the unethical commercialization of medicines in third world countries by Gilead Sciences at http://blog.bioethics.net/2006/02/aids-drug-treatment-access-walking.html. If you have come this far, it sure will make a compelling read.
posted by littlecow at
11:14 PM
![]()
![]()

2 Comments:
ah yes, i was just going to mention some stinker facts about the trials when i came to the last paragraph. clinical trials are ethical disasters, and when conducted in third world countries, all the more so. but you know that.
just wanted to say : awesome. after working in an intervention team for HIV awareness and prevention, i have a new appreciation for people who are bothered enough to speak up about this mess.
great going :)
@m.:
>after working in an intervention team for HIV awareness
Good! Keep up the nice work.
I am curious to know what was done here. Where was this? India? What are the prospects for an improvement of the situation in India? Do people/government recognize the dire situation here - that India has the largest number of AIDS patients outside of Africa?
I am aware of the dubious nature of trials. One question that eludes me is the nature of ethical standards adopted by Indian companies like Reddy's laboratories. Are they any better than the foreign companies?
Post a Comment
Subscribe to Post Comments [Atom]
<< Home